A set of attitudes, habits, or possessions associated with a particular person or group. and such attitudes, etc, are regarded as fashionable or desirable.
Final message
Communicable disease need not be an Infectious disease like covid. The word “Communicable” shall soon convey a new meaning, to the enlightened. Adverse life styles ,disseminated into the community that vigorously propagate CVD, has every reason to be referred to as a ‘Neo non-infectious pandemic”
Postamble
In the strict sense, CVD is not a communicable disease ,rather the risk factors are …but technically it is.
Here is a pleasant surprise, a collectors issue of NEJM year book 2023, is made available free (even for non subscribers, in its website) .It is fascinating to know how fast the Internal medicine has grown. For the busy cardiologists, this will a be refreshing reminder, that there are other important organs and specialties do exist in medicine , with equal breakthroughs and Innovations.
It is indeed an amazing , whirlwind tour of medicine for all those who see medical science as single holistic specialty. It has articles, ranging from from simple clinical studies on postpartum hemorrhage (E-MOTIVE study) from deep inside Africa by Melinda Gate foundation, to Dupilumab for COPD, a stunning monoclonal antibody inhibitor of IL-4 for COPD exacerbations. Shortening tuberculosis treatment with a strategy involving initial treatment with an 8-week Bedaquiline-linezolid regimen (TRUNCATE-TB study) is also a revelation.
Of-course, the mandatory cardiac topics do find a prominent place including the currently omnipresent drug GLP agonist Semaglutide for HFpEF (STEP-HFpEF study). Baxdrostat, an Aldosterone synthase antagonist for treatment-resistant Hypertension, appears promising (BrigHTN).
Final message
However, the crowning glory among all articles appear towards the end of the document, titled Combating misinformation as a core Function of Public Health.
Let me share the link to this PDF document here. Hope it allows open access and there are no copyright issues. Notable articles of 2023 from NEJM .
Statins belong to a group of drugs, stolen and reengineered from the blueprint of natural Chinese red yeast rice (Monocoline K) in the late 1980s. The rest is the remarkable history in the pharma industry.
Statins directly interrupt the cholesterol synthesis by blocking HMG-CoA within the hepatocytes. It significantly lowers the LDL, fights human vascular atherosclerosis. It makes the plaque either regress, prevent progress, make it harder and in the process make them less vulnerable . There are innumerable studies that document the evidence. Statin has become a must-prescribe drug in any one with clinically established CAD or even in concealed CAD. Guidelines are available to prescribe statins various intensity, depending on the risk profile.
Which statin ?
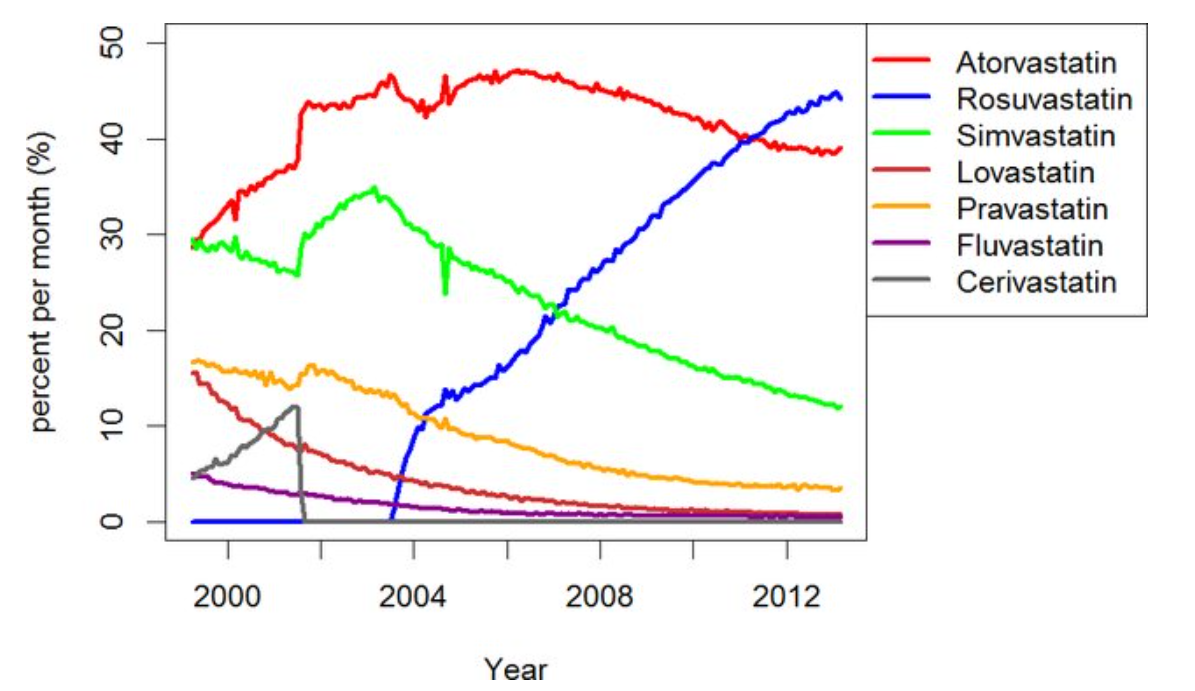
There has been a long list of statins. Many of them have retired from the ring .Currently, the fight is between Atorvastatin, a Rosuvastatin. Like Pepsi vs. Coke.
Note the graphic ,A meteoric rise of one drug since 2005 . (Can you guess the reason ?)
ATRORVA or ROSUVAWhich one should I choose ?
There is very little “one to one” comparison study between Rosuvastatin and Atorvastatin .The gap in the pros and cons are narrow. Following points are observed, without much dispute.
No one is dare enough to give strong verdict . Surprised to find one this month. BMJ has come out with a possible answer. It is called LODESTAR trial (Ref 1)
Mechanism of new onset diabetes with statins (REF 3)
It can be 7% with Rosuvastatin (less with Atorvastatin). We think, statins act primarily within the hepatocytes where cholesterol synthesis takes place, but they also have an eye on the pancreatic β-cells as well. It down-regulates GLUT-4 in adipocytes, and results in compromised insulin signalling. Furthermore, statins’ impact on epigenetics may also contribute to statin-induced T2DM via differential expression of microRNAs.
Mechanism of cataract with statins (Ref 2)
The cells lining that line the lens are dynamic and require cholesterol on a day-to-day basis. Statins inhibit proper epithelial cell development within the crystalline lens, where cholesterol biosynthesis is critical to maintain transparency and structure of the lens.
Final message
So, is it Atorvastatin or Rosuvastatin? It is left to you.
Mind you, “no statin at all” is the best option if circumstances and risk profile allows. Statins are never considered life-saving staple drugs in our fight with CAD and atherosclerosis. We, along with our scientists might may make you feel like that. Lipids can be controlled within desirable means exclusively with diet and exercise in most of the population* .
(*Forget about statins in the last 5000 years of known human existence, so many great people have lived a long and successful life in this world, without even knowing there is an organ called the heart that is responsible for the circulatory system)
This quote is being sent for the annual meet of “Right care movement” I know ,this can sound outrageous, permissble limits of abuse ? Up to 2% or 5% ? Let it be anything . Meanwhile try to enlighten yourself , the key differences between misuse & abuse.
This sound bite is regularly uttered by all academic leads in any university or medical school. I don’t know, why this bothers me. Looking back, many of our mentors & professors never had any great publications. Still, they were extraordinary teachers and wonderful clinicians with great wisdom. They created generations of high-quality doctors who are present all over the globe now. Is scientific publication that important in a doctor’s life? After pondering for quite some time, got a hazy answer to that query in one of my sleepless early morning academic dreams.
Hippocrates was one of the applicants for the post of professor of medicine at Harvard medical school.His application was rejected for a dismally low H index. The reluctant father of medicine tried to impress the authorities, by telling them that his experience was vast and used to teach medicine 2000 years ago, well before their country USA was discovered. The father of medicine almost begged to reconsider their decision.The miffed Harvard academic office ridiculed the old man and insisted nothing will work, except a minimum H index of 50 or atleast 10 papers as first author in a peer reviewed high Impact factor journal. A dejected Hippocrates returned to Kos islands and asked his new generation fellows, what is this H index and Impact factor stuff ? His students were worried about their guru’s ignorance. They some how convinced the greatest ever medical teacher to urgently subscribe for a platinum membership of a premium medical authourship services located in the Boston suburb and fixed a 30 day deadline for his first manuscript.
Now, let us travel back in time,2000 years ago to this picturesque nation, Kos islands in the Aegean sea,. This is where Hippocrates taught lessons under his favorite tree. No teaching apps, No 4k audiovisuals, The humble noise from within his lips became great wisdom thoughts. All that students had were set of ears to hear him. Hippocrates became the celebrated father of medicine for two reasons. He was the first to dispute the then-prevailing thoughts about human health and disease. He first proposed for every illness there is a hidden reason ie the beginning scientific basis. He insisted and negated the idea that diseases are bestowed upon by evil forces and spirits. The second one is more important. He realized knowledge, skill, and power are a deadly mix for the healing industry if they lack responsibility. He foresaw non-academic factors that will try to challenge the integrity of medical professionals and the health care delivery systems. It is astonishing to note how he could predict this 2000 years ago and wrote the behavior code for medical professionals which has become immortal.
How to grade the quality of medical professionals?
Scientific publication is just one of the indices of quality assessment for medical professionals. Grading them based on a few manufactured rating systems is beginning to look like an academic comical. There are many more visible and invisible, quantifiable and non-quantifiable quality assessment parameters that deserve attention.
Research & Innovations are indeed the pivotal pillars that take us to newer frontiers of medicine. But, It is explicitly clear now, the prime purpose of research is definitely not aimed at the growth of science. It is more of a survival tool, intertwined with commerce, status symbol, pride, peer pressure, self-esteem, rivalry, or just a filler for CV.
Final message
Blanket statements like Publish or perish at any cost could be a dangerous doctrine to adopt in medical education which is essentially about healing and caring (& whenever possible, curing). In one sense, medical teaching is little to do with research. Many of the great professors in our country never published a single paper. Unfortunately, research and teaching have been made to look inseparable. Beware, history has repeatedly taught us medical professionals need not be hyper-intelligent. They need to be just wise, men /women of integrity, enriched with sincerity, righteousness. Proper consumption of knowledge is much more important than the creation of it. Let us hope the future will be at least as perfect as the past.
Postamble
My H index stands at 15, I must confess I am confused a lot. Should I bother for more, or be just be happy to reach the H index of our mentor and father of medicine, which is numero Zero, and propagate his work.
2.Academic excellence does not always require publication Ernest L Boyer argued in his 1990 book, Scholarship Reconsidered: Priorities for the professoriate,(BoyerScholarshipReconsidered)
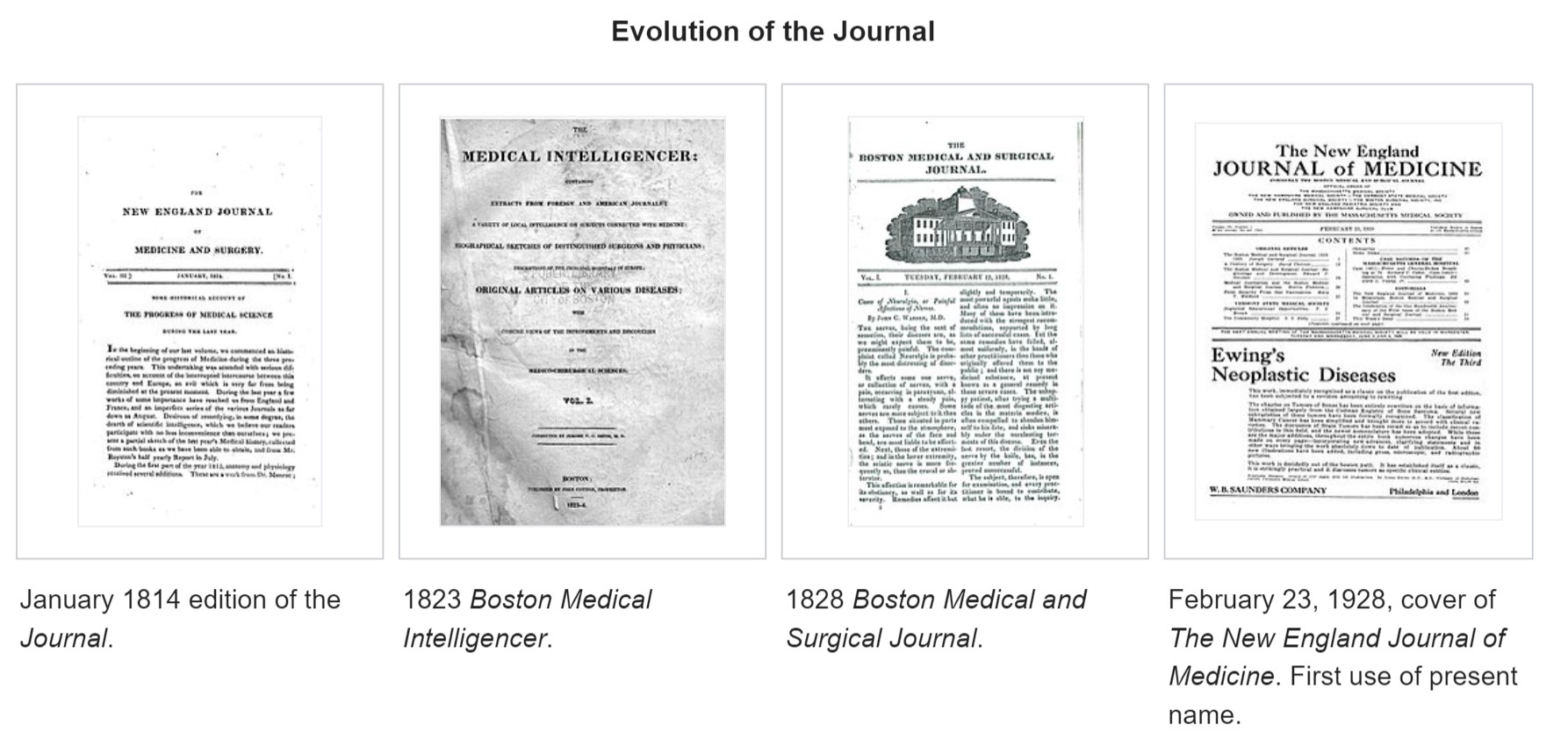
The New England Journal of Medicine (NEJM) the premier journal in medicine originated two centuries ago, in 1811, when John Collins Warren, a Boston physician, along with James Jackson, submitted a formal prospectus to establish the New England Journal of Medicine and Surgery and Collateral Branches of Science as a medical and philosophical journal.
Subsequently, the Massachusetts Medical Society (MMS) purchased the Journal for US$1 and, in 1928, renamed it to The New England Journal of Medicine.
NEJM’s New Journey
It is 2022, after 200 years of providing explosive knowledge in medical science, MMS starts a new journal, fresh and bold. It is called NEJM Evidence. Can you guess, what is the need for such a journal now? I think the most battered word in science in current times is probably “ evidence”. It has a unique character of appearing most sacred as well as scandalous at the same time.
NEJM has remained the torchbearer of almost all advances in the medical field seen in the last two centuries. It is heartening to note the newborn is named as NEJM evidence. It has come at a critical juncture. I am sure, everyone will acknowledge that we are at difficult crossroads. Overwhelmed with unregulated scientific discoveries and publications, struggling to deal with self-inflicted knowledge pandemic. In the process, we have lost “not only” the ability to ignore trivial health issues “but also” failed to provide simple, cost-effective care to the real patients who desperately need it.
Let us hope, (& wish,) NEJM’s new prodigy will guide medical science towards a successful, meaningful, and ethically fulfilling journey for mankind. Meanwhile, let us pray for every medical scientist to be blessed with the required strength and courage to steer in the right direction, weeding off both academic and non-academic contaminants.
When we get contaminated with excess knowledge , we lose our ability to think ! & Common sense is the casuality . . .
Human beings differ from other forms of life by their sixth sense . Our planet is few billion years old . Life came into existence over a million years ago .Our life has evolved over many thousands of years .The average life span of human race is 75 years . We need to realise , our life constitutes only a fraction of our planet’s life (<.0000001% ) . A may fly , which lives a life of less than a day , does it in style , looking for the light throughout the night , says good bye , to earth by morning leaving it unharmed . Actually , in terms of time , the life of the fly is just a fraction less than human life span , when compared to our planet’s life !
When these children are longing for food , some of earthly humans go to spend millions for obesity surgery ! That is the progress of knowledge driven society . . .
It is extremely common to experience the following scenario in any corporate hospitals of both developing and developed country .A uninsured or half insured ! person is refused entry into a hospital even for an emergency care while a wealthy person is lying comfortably watching TV in a five star suit of the same hospital after an inappropriate coronary angioplasty for an innocuous lesion of his heart !
The irony is , in this short span of earthly life , we want to prevail over the nature and conquer the planet . God is watching this human behavior silently . And he is smiling . . .
With all our knowledge base , modern science have done the maximum possible damage to our planet .We have made many lives extinct. If we tend to think , with the help of 6th sense we can become immortal , it would be the ultimate foolishness. When every one of us , is obsessed with our own health , we are deaf to the silent cries of our beloved planet earth .
Now , all of a sudden we realise all the accumulated knowledge & development has actually worked against us. We find our knowledge is dissociating our thoughts and now , we are fighting vigorously over acquiring the rights to damage our planet .
So it seems , the more we learn, less wisdom we have ! We may need to learn important lessons of living from all those species which do not boast to have the 6th sense !
Read a related article , excellent one published in British medical journal nearly 2 decades ago
Pessimism, from the Latin pessimus (worst), is a state of mind which negatively colors the perception of life, especially with regard to future events.
Understanding pessimism is not that simple . Some people argue optimism represents a strong mind while a pessimism is the domain of the weak . But it is not necessarily true. Both pessimist and optimist are unreal , and playing the dangerous game of predicting the future. So realism is the answer .
In this era of information highways , commercial exploitation of science , our thought process is grossly determined by our perception of events.We hardly have an intention or time to analyse our thought process.
An optimist ( Rather , unregulated optimist ! ) is a person who welcomes any growth good or bad.*
A pessimist is a person who welcomes only good growth.*
So how to identify good growth ? That is the million dollar question!
Many of the optimists may not bother about the final outcome of a treatment *
A pessimist bothers only about that .
An optimist rarely asks questions, blindly accepts every thing !
A pessimist never believes any thing !
Actually the fundamental principle of scientific medicine lies in proving the null hypothesis null and void.Any treatment is useless until proved other wise . So pessimist can be argued to follow true science , while many of the hardcore optimists are blind believers ..
*It may be a harsh way of interpreting an optimist but uncontrolled optimism has played havoc in our patients like many of the failed treatments (Some of them released prematurely into patient domain has killed many lives . Power of positive thinking should be within the realms of scientific feasibility !
So in our journey to conquer human health , we may proceed with an optimistic mind and a pessimistic eyes !
This understanding is all the more important in this era of contaminated science .It is a well known fact , now last 50 years of planet earth has inflicted the maximum damage to ourselves than our ancestors did in 5000 years. That’s why we are compelled to meet at Copenhagen .(We never learn from our mistakes, that’s a different story !) .
There is definite and urgent need for world summit on cleansing the medical science from the clutches of commerce and ignorance . A medical green house effect, with dangerous holes in health care is imposing on us (Another pessimistic thought . . . of course in the interest of human kind !)
World health organization , a sleeping giant has to be awakened on this issue
Final message:
Mankind has evolved over many millenniums , probably with a sole purpose of living , that is reproduction and propagation of our genre without harming the environment and other species.
Unrestricted and unregulated growth of any kind is dangerous we call it as malignancy in pathology .In science , we tend to call it a” great future ”
Our sixth sense* has outgrown miserably out of reality , as have we decided to take on the nature and GOD .Now , many developing country men do not believe in death .They are fighting a losing battle against the God. And they suffer with escalating health costs of keeping the elderly , alive who are knocking at the doors of heaven or hell . The same countries, which deny funds for curable illnesses of the poor is a different story altogether !
The principle of modern medicine would ideally be
Reduce human suffering irrespective of economic status
Curing a illness if there is a cure
Prolonging life if there is useful purpose
Allow a good quality death if there is no cure.
Most importantly , prey to god give us strength and capacity to identify which is good and which is bad for our patients .
Read and learn for a complete guide on optimism and pessimism
* It is important to recognise , the same sixth sense has made it possible to share our views through a great tool of Internet . So we should not be against the growth of science but against the misuses and wrong interpretations of it .
What are the fundamental difference between randomised studies and observational studies ?
New discoveries come from shrewed observations made in bedside or labside while , randomised studies evaluate these discoveries for it’s effectiveness or futileness .
Let us realise , RCTs primarily never contribute to generation of original concepts or discoveries ! .It is a statistical tool to assess an observation .
Click below to reach the excellent knowledge source on above the issue .
The fact that observational studies are done with open eyes & mind , it is obvious it demands intense conceptualization and thinking .
Blinded studies are mechanical studies . It is pure statistical research . It requires no thinking , medical mind , in fact one can do it with eyes closed as it is a strict protocol driven , even a non medical men can do a medical research , while it needs a alert mind to do a observational study .
Observational studies , especialy when done retrospectively has zero bias as the case selection and the potential intervention are completed even before the research question is raised. In fact many of the greatest medical breakthrough comes from retrospective analysis. Of course this has to be proved prospectively preferably in a randomised fashion.
So , we the medical professionals , shall do great observational research with open eyes and mind and let the the statisiticins do the outcome analysis blind folded .
If the core medical professionals are bothered more about randomised blinded studies ,which is meant only for evaluation purposes , the future of intellectual medical research is going to be in jeopardy!
Do 64slice MDCT in all patients who has a coronary event and follow it up with catheter based CAG.
Use liberally the new biochemical marker , serum B-naturetic peptide (BNP) to diagnose cardiac failure in lieu of basal auscultation.
Advice cardiac resynchronisation therapy in all patients who are in class 4 cardiac failure with a wide qrs complex .
As it is may be considered a crime to administer empirical heparin, do ventilation perfusion scan in all cases with suspected pulmonary embolism.
Do serial CPK MB and troponin levels in all patients with well established STEMI .
Open up all occluded coronary arteries irrespective of symptoms and muscle viability.
Consider ablation of pulmonary veins as an initial strategy in patients with recurrent idiopathic AF. If it is not feasible atleast occlude their left atrial appendage with watch man device.
Never tell your patients the truths about the diet , exercise & lifestyle modification (That can cure most of the early hypertension) . Instead encourage the use of newest ARBs or even try direct renin antoagonists to treat all those patients in stage 1 hypertension.
Avoid regular heparin in acute coronary syndromes as it is a disgrace to use it in today’s world. Replace all prescription of heparin with enoxaparine or still better , fondaparinux whenever possible.
Finally never discharge a heftily insured patient until he completes all the cardiology investigations that are available in your hospital .
Coming soon : 10 more ways to increase cost of cardiology care . . .beyond common man’s reach
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.