Preamble : The Lubs & Dubs
The lubs and dubs, along with some added sounds are the only language, the heart can speak in health and distress. It’s a worrying story altogether, gradually many of us are becoming “cardiac illiterates” as we struggle to read , its gentle communication. it is not our fault. Stethoscopes are reduced to become a social marker of being a doctor. We may excuse ourselves, even if we can’t differentiate a systolic from diastolic murmur, after all, hand held echo machines, instantly tell the diagnosis.
( After reading this article, fellows are expected to understand why the first heart sound in MR (ie the lubs,) are mostly soft, some times normal or even loud in certain conditions)
Now, let us go to the mitral valve dynamics
How many of us are aware, there is a big science of physics and biology operating when the mitral valve perfectly closes at the level of the annulus, with each systole , balancing different sets of known and unknown forces.
In this article, we will see how these two sets of forces mitral valve tethering and closing forces balance out each other to seal the mitral valve and what happens when the forces begin to fight each other.
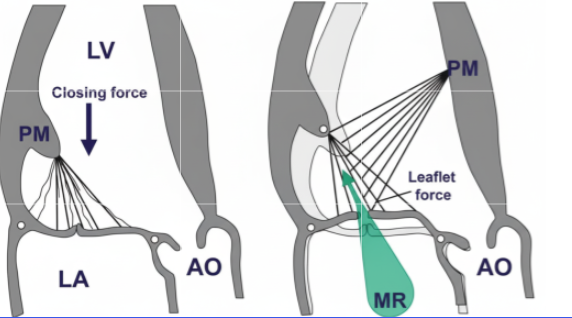
Balance of Tethering and Closing Forces in Mitral Valve Coaptation
The mitral valve (MV) coaptation refers to the edge-to-edge apposition of the anterior and posterior leaflets during systole, ensuring a competent seal to prevent regurgitation. This process is governed by a delicate balance between tethering forces (which restrain leaflet motion to prevent prolapse into the left atrium) and closing forces (which approximate the leaflets for sealing).
- Tethering forces: These are primarily transmitted through the chordae tendineae from the papillary muscles (PMs) to the leaflet free edges and bellies, pulling the leaflets apically and laterally toward the left ventricular (LV) apex. They arise from:
- Closing forces: These are driven by the transmitral pressure gradient during systole, where rising LV pressure (generated by LV contraction) exceeds left atrial (LA) pressure, pushing the leaflets together. The force is proportional to the LV dP/dt (rate of pressure rise) and peaks in midsystole.
- Balancing mechanism: Coaptation occurs when closing forces overcome tethering, enabling leaflets to meet with sufficient overlap (coaptation length >8 mm typically). Imbalance favors regurgitation: excessive tethering (e.g., from PM displacement) causes apical tenting and incomplete closure; insufficient closing (e.g., low LV contractility) fails to seal the orifice. In health, the forces are synchronized with systole, with closing forces dominating midsystole to minimize the effective regurgitant orifice area (EROA).
Paradoxes in the Balancing Mechanism
MV mechanics exhibit several counterintuitive paradoxes, where adaptive or dysfunctional responses lead to outcomes opposite to expectations. These highlight the interplay of geometry, contractility, and force transmission:
- Paradoxical systolic PM elongation: Normally, PMs shorten during systole (1 cm) to offset annular descent and maintain annulopapillary balance. Post-myocardial infarction (MI), scarred or ischemic PMs paradoxically elongate driven by transmitral pressure tension. This decreases annulopapillary distance, attenuates tethering, and reduces MR severity—contrary to the intuition that PM weakness worsens regurgitation. However, extreme elongation risks leaflet prolapse, flipping the paradox to increased MR.
- PM dysfunction attenuating ischemic MR: In isolated dysfunction, reduced PM contraction intuitively increases slack chordae and prolapse risk. Yet, in localized basal inferior LV remodeling, PM dysfunction (measured as reduced longitudinal systolic strain) inversely correlates with MR fraction attenuating MR by limiting excessive tethering. This holds only with certain level of remodeling . Gross and asymmetrical remodeling can exaggerate tethering and increase the MR.
- Dynamic EROA reduction despite peak driving pressure: MR often peaks early systole (when closing forces are low and tethering dominates) but paradoxically decreases midsystole, even as LV pressure (driving force) maximizes. This occurs because rising closing forces (transmitral gradient) overcome tethering, shrinking the orifice mimicking reduced regurgitation when it should worsen.Thgis mechansim can some times seen when MR jet is bi-fid in doppler tracing.
- Imbalanced chordal forces causing focal prolapse: In acute ischemic MR (e.g., posterior wall ischemia), tethering redistributes unevenly: tension drops in ischemic-side chordae but rises on the nonischemic side causing focal tenting and relative prolapse on the ischemic commissure. This creates an eccentric jet despite global LV contraction.
This article clearly tells us that the forces acting on the mitral valve apparatus are so complex. The conceptual model of tethering and closing forces may be oversimplified. There are variable interactions between them. More importantly, the atrial forces also influence and intrude into these forces. Realize that MV competence is not just about force magnitude but their vectorial distribution and timing, often amplified by LV geometry changes.
Final message
As cardiologists and surgeons, we must realize the fact, how important it is to analyze both anatomy and the physiological impact when we rush to clip, cut, or repair it with annuloplasty and subvalvular interventions.
*Sometimes, it might even be tempting to do mitral valve replacement, even when it is not indicated, because we need not bother about all these dizzy mechanics and physics of MR jet forces.














{kind=link}