September 19, 2008 by dr s venkatesan
Indication for thrombolysis in ST elevation MI is mainly determined by clinical and ECG features. ST elevation of more than 1mm in two consecutive leads with a clinical suspicion of acute coronary event demands immediate thrombolysis.
Early repolarisation syndrome(ERS) is a is typical mimicker of STEMI . In ERS , ST segment elevation occurs in many leads especially precardial .This entity is estimated to occur in nearly 3-5% of population where a genetic variation in the potassium channel activation is reported.

If they land in ER with some sort of chest pain , chances are high for labelling them as ACS . It is not uncommon for CCU physicians to witness an ERS being lysed . Even in many of the land mark trials (ISIS ) there has been many inappropriate thrombolysis , recognised later on.
What can really happen if you thromolyse them inadvertently ?
Generally nothing happens . But they are exposed to the risk of thromolysis. The ECG changes persist. And troponin will be negative and echocardiogram will not reveal any wall motion defect.
Are we legally liable if a patient with ERS was thrombolysed and he ends up with a bleeding complication like stroke ?
While the physician may feel guilty , there is no reasons for him to feel so.The guidelines are kept little lineant for the indication for thromolysis. When we are promoting a strategy of early thrombolyis on a population based approach in STEMI , there is bound to have a overlap with normality .The benefits out of early thrombolysis for eligible patients for outweigh the few inappropriate thromolysis.
When you want to catch a real criminal it is unavoidable, one gets hold of all suspected criminals before letting them free . Unfortunately in this exercise , some of the innocent might experience intimidation or even a injury at the hands of law enforcers.
Similarly if a patient with ERS develop a severe esophageal spasm and typical angina like chest pain he is absolutely certain to receive thrombolysis. (Troponin, CPK come later , and the results never veto the clinical and ECG criteria ,except probably in LBBB) .Many times critical time dependent decisions are prone for errors in CCU. So it may be unscientific to ask why an ERS was thrombolysed !
How can one prevent inadvertent thrombolysis in ERS ?
Always ask for the previously recorded ECGs .If it is available and look exactly similar to the current ECG chances are unlikely for ACS. In ERS ST segment is generally concavity upwards . ACC/AHA guideline for STEMI ,is aware of this fact , but still advices thrombolysis for all ST elevation irrespective of the morphology of ST segment elevation. This is propably intentional, not to incorporate morphology cirteria of ST elevation for thromolysis .It would potentially make many true STEMIs diagnosed falsely as ERS and deny thrombolysis.
What is the latest news about ERS ?
Now data are coming up, ERS is not entirely benign condition.Some of them ( Even a fraction of ERS population could be a significant number) can have a overlap between Brugada syndrome and they could be prone for dangerous ventricular arrhythmia when challanged with ischemic or other stress.
Posted in cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acc stemi guidelines, acc.aha, american college of cardioogy, bmj, brugada syndrome, cardiology, ccu, chest pain, coronary care, drsvenkatesan, early repolarisation syndrome, emergency room, ers, jama, legal medicine, medical error, nejm, stemi, streptokinase, thrombolysis | 2 Comments »
September 18, 2008 by dr s venkatesan
The pressure tracing between two chambers of the heart are distinctly different .
Apart from the magnitude of the pressure ,(LV at systemic pressure ) The morphology also changes.
- RV pressure curve is triangular in shape,
- Upstroke is not rapid , (Low dp/dt)
- There is no sustained peak ,
- There is an early fall and
- The pressure falls to zero which never happens in LV.
Contary to this LV pressure curve is bullet shaped, with a rapid upstroke, sustained peak, fall later, and does not touch zero.

RV/LV pressure curves in normal persons .Adapted from , Curtiss 1975 Circulation
Note : The shapes of RV curve will change in pathological states.Example in TOF, large VSD there will be left ventricularisation of RV pressure wave forms. Also in pulmonary hypertension RV pressure may mimic a LV curve.
Posted in Hemodynamics, Tutorial in clinical cardiology | Tagged aortic pressure, cardiology, cath lab, drsvenkatesan, hang out interval, Hemodynamics, left ventricle, pressure curve, pressure tracing, pulmonary artery, right ventricle | 2 Comments »
September 18, 2008 by dr s venkatesan
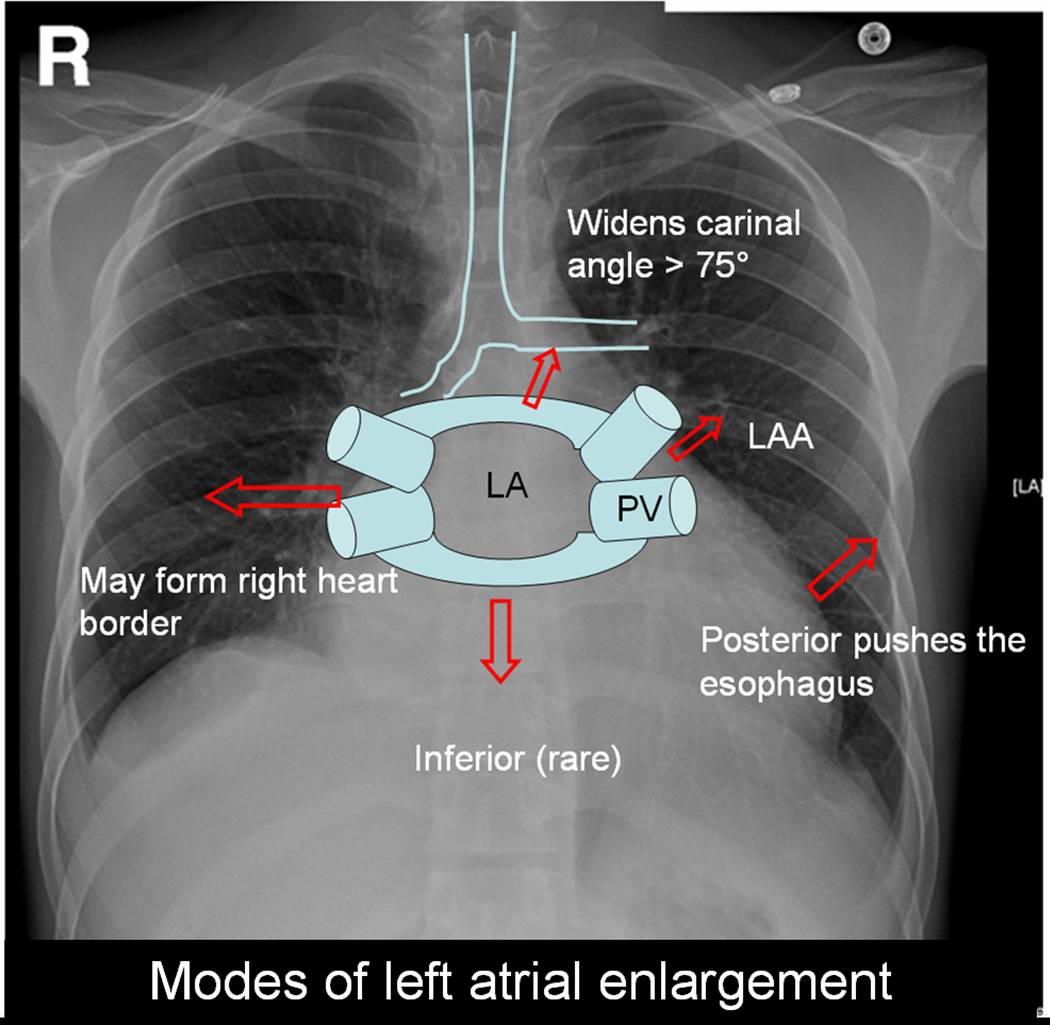
Left atrium is the posterior most chamber of the heart. It is almost a mid line structure. The normal size of left atrium is about 4 / 4 cm. Normal left atrial volume is 46ml in men and 38 ml in women .(Atrial volume in a normal adult population by two-dimensional echocardiography Y Wang, Chest, Vol 86, 595-601.) Left atrium is not an easy chamber to identify in the X ray chest as it does not form the cardiac border.( Except a small circumference of left atrial appendage.(LAA)
Left atrium can enlarge in multiple directions.Generally it dilates in the path of least resistance.

- It is believed left atrial appendage enlargement occur early . LAA enlargemnet seen as a fullness beneath the pulmonary artery shadow. It may be the earliest finding of LAE in X ray. ( This may appear as straight left heart border , as in classical mitral stenosis where MPA is also enlarged). The LAA enlargement is not necessarily in in proportion with LAE.
- LA could also enlarge posteriorly by pushing the esophagus towards the spine.This is visible only in barium swallow.
- Then LA can enlarge either to left or right ( Usually towards right) and reach the right heart border or over shoot it and form the right heart border by itself.This occurs very late in the course.
- The other direction LA goes on to enlarge is superiorly. When LA enlarges superiorly it hits on the left main bronchus and lifts it.This is measured by the widened subcarinal angle which is normally less than 75 degrees.
- LA can enlarge anteriorly sometimes , but it is resisted by right ventricle but rarely right ventricle yields to the LA push and produce a left parasternal lift which could be mistaken for RV enlargement.
- Inferior enlargement can not happen in a significant way as it is limited by the AV groove and strong fibrous skeleton.
With the advent of echocardiography X ray assessment of LA is redundant .(Academic value and in fellows training programs).The upper limit of normal LA size is around 4.5cm.
LA enlargement is commonly seen in
- Rheumatic mitral stenosis, regurgitation. Gross enlargement up to 10 cms are common.
- Hypertensive heart disese.
- Cardiomyopathy, especially restrictive where both atria enlarge.
In all these conditions if atrial fibrillation occurs LA size increases further.
Posted in Cardiology - Clinical, X ray | Tagged annals of radiology, atrium, barium swallow, cardiology, carinal angle, chambers of heart, drsvenkatesan, lancet, left atrial volume, left atrium, left heart border, mitral stenosis, nejm, radiograpgy, radiology, rheumatic heart disease, right heart border, X ray | 1 Comment »
September 14, 2008 by dr s venkatesan

Chest pain is one of the commonest presenting symptom in any hospital both as an emergency or non emergency. Reaching an accurate diagnosis is very important. The main purpose of evaluation of chest pain is to recognise it as cardiac or non cardiac origin . Cardiac chest pain almost always means ischemic chest pain . That is called angina. (Of course there are few important causes for non ischemic cardiac chest pain which Will be discussed later).
Standard features of typical angina.

Chest pain which falls short of typical features are called atypical chest pain . Some recommend at least three typical features to label it as angina.
After the clinical examination patients should be categorised in one of the following .
- Typical angina
-
Atypical chest pain
-
Non cardiac chest pain** Non cardiac chest pain is not a diagnosis. Any physician (or a specialist) should take some effort to localise it. (Muscle, nerve , pleura , anxiety etc) . But generally once these patients are ruled out of cardiac pain they become less special and are simply referred back to their family physician, only to return back with another cardiac pseudo-emergency in a different hospital .
Why we are diagnosing atypical chest pain liberally ?
Currently more number of patients as well as the physicians are aware of the looming epidemic of CAD. The other major reason is the lack of application of mind during foirst clinical appraisal and examination. Many of the patients with non cardiac chest pain (Muscle, nerve , pleura ) are termed as atypical chest pain. Though some of the popular texts use atypical chest pain and non cardiac chest pain interchangeably , it is not correct to do so. For example don’t ever label a patient with chest pain with chest wall tenderness as atypical chest pain and order a cardiac work up .It is a poor model to emulate , that consumes time and resources!.Instead they should be diagnosed a confident non cardiac chest pain and dealt properly.

Once a patient is diagnosed atypical chest pain what’s next ?
They should get a complete physical examination,ECG, and undergo exercise stress test. In the screening of CAD , angina can be termed a hard sign, atypical chest pain is a soft sign, resting ECG is surprisingly a soft sign again (unless you record it during chest pain). Exercise stress testing is the ideal investigation in evaluation of chestpain.( 70-80% accuracy). This can be improved upon by Thallium, SPECT, stress echo etc. As of now coronary angiogram is considered the ultimate gold standard (Not pure gold !) to rule out CAD.
It is also worthwhile to remember non anginal chest pain can also be an emergency and life threatening
- Pulmonary embolism
- Pneumothorax
- Thoracic tumors
- Aortic aneurysm (Dissection and non dissection) The list is not exclusive
Final message
What do we really mean by atypical chest pain ?
In reality we don’t mean any thing !
When a cardiac physician is confused or rather , unable to rule out angina , at the same time he is not confident of calling it as non cardiac chest pain, he has the luxury of using this terminology . It is obvious this terminology should minimally be used. Once diagnosed these patients can’t carry on with this tag for long. They should be reinvestigated , (Right from history and clinical ex) .They should either enter the cardiac work up protocol or a non cardiac source for pain should be fixed immediately.
Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, angina, annals of internal medicine, approach to chest pain, atypical angina, atypical chest pain, bmj, cardiology, chest pain, chest wall tenderness, coronary, drsvenkatesan, ECG, emergency room, er, Heberdens, jama, lancet, myalgia, nejm, non cardaic chest pain, troponin, unstable angina | 4 Comments »
September 11, 2008 by dr s venkatesan
Infective endocarditis is a serious clinical cardiac problem. The disease has evolved over many decades and now we are witnessing the most virulent forms of the disease . Infection of heart , can occur in a native healthy valve, native diseased valve, or a prosthetic valve. Further, IE can occur either as an acute (usually non diseased valve) , or sub acute form (usually in diseased valve).The changing microbial pattern has made this entity very complex. The vigorous treatment protocols are available for IE. Still the prognosis and outcome with medical management is dismal even in best centers.So the role of surgery in IE has increased over the years.We propose here, a radically different approach to the problem.
Traditionally there is a set of criteria for surgery in IE : These include
- Abscess formation
- Worsening valve lesion
- Refractory cardiac failure
- Persistent fever even after 2 weeks of appropriate and adequate anti microbial therapy .
- Vegetation of more than 10mm size.
- Failed medical treatment
(The list is not exclusive)
In any large tertiary hospital series, if you apply the above rule more than 50 % of all patients with IE will be the candidates for immediate surgery.
In the remaining 50% the mortality in medical management is very high. The reason being, the medical treatment is often prolonged over weeks. Many of the complications occur during the course of medical treatment.The common ones are abscess formation, embolic episodes, renal failure etc.Once a complication set in we call it as failed medical treatment and ask our surgical colleagues to operate.By this time patient’s general condition deteriorates and either the surgeon refuses to take up the case or patient dies on the table.
So the key point is , failure of medical treatment is so common , it is simply not acceptable to delay the surgery in these patients as majority of them are doomed to fail the trial of medical therapy.

What is the incidence of failed medical management, how to recognise it ? what is the impact of recognising it late ?
- Failed medical therapy is around 60-70% even in best centers.
- Failed medical patients constitute the greatest surgical risk .
- So it is proposed all IE patients should be triaged early and the dominant theme should be surgery (Commonly valve replacement, or valve repair) .
- If there is large vegetation surgery may be done for the sole purpose of physical removal of the vegetation*.
Final message
In Infective endocarditis experience has taught us, surgery should be the default management protocol and medical therapy should be offered to selected few who don’t require surgery.This is especially true in preexisting rheumatic valve disease.
*The fundamental principle of management of infectious diseases, state that when there is a resistant focus of infection .Always remove the focus whenever possible.
Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged antibiotics, aortic valve, cardiology, cdc, chordal rupture, culture, drsvenkatesan, duke's, durant, fuo, heart, infectious disease, infective endocarditis, micro biology, mitral valve, myocardial abscess, prolonged fever, prosthetic valve, puo, staphylococcus, valve replacement, valvular heart disese, vancomycin, vegetations, viridans, von ryan | 1 Comment »
September 10, 2008 by dr s venkatesan
This is a 15-year-old post about LVH, written in 2008. Few of my colleagues, now agree with this, still hesitate to oblige in the open, suggesting it is too good to be true! Re-posting it for your own assessment. Surprised, why cardiology community didn’t consider this observation worthy to pursue.
Advantages of Left ventricular hypertrophy (LVH)
Left ventricular hypertrophy is one of the most common clinical cardiac entity.It is recognised either by ECG or echocardiography.LVH has a unique place in cardiology as it can imply a grossly pathological state or a marker of healthy heart as in physiological hypertrophy in athletes.
Logic would suggest, in this era of stem cells and nano medicine , every muscle fibre in ventricle is worth in gold !. So when the nature provides an extra reserve of myocardium in the form of LVH one should welcome it , if otherwise not harmful.

Is LVH due to systemic hypertension benign ?
Not really, LVH has been shown to be an independent cardiac risk factor. (The famous Framingham study)Further LVH can result in diastolic dysfunction and the risk of cardiac failure increases.
But in spite of these observations, an astute clinician with considerable experience will appreciate , patients with LVH fare better during an acute coronary syndrome !
This has been a consistent clinical observation . (Shall we call it as class C . ACC /AHA evidence ? )
Is LVH an asset during ACS ?
- A hypertrophied heart takes ischemic injury very easy , it doesn’t really hurt much . Another possibility is that in LVH myocytes are relatively resistant to hypoxia .
- Patients with LVH rarely show significant wall motion defect following an STEMI.This is probably because the full thickness transmural necrosis is almost never possible even if extensive MI occurs.
- This is also reflected in ECG as these patients rarely develop q waves in following STEMI .
- Persistent ST elevation and failed thrombolysis is very uncommon in pateints with LVH.
- LVH provides a relative immunity against development of cardiogenic shock . It requires 40% of LV mass destruction to produce cardiogenic shock.This can rarely happen in LVH. In a long term analysis we have found none of the patient with LVH developed cardiogenic shock following STEMI.
- LVH patients are also protected against development of free wall rupture.
Concluding message
“Lack of published evidence is the weakest evidence to dismiss a true myth”
LVH , either pathological or physiological, has a hitherto unreported beneficial effect.It acts as a myocardial reserve and helps limit the impact of STEMI.
Posted in Cardiology - Clinical, cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, atheletes heart, cardiac failure, cardiac reserve, cardiology, coronary, framingham study, hypertension, left ventricular hypertrophy, LV mass, lvh, myocardium, nstemi, pci, ptca, stemi | 1 Comment »
September 10, 2008 by dr s venkatesan
Intra coronary thrombosis is the sine qua non of acute coronary syndrome ( Both STEMI and NSTEMI.) But thrombolysis is the specific therapy in STEMI and is contraindicated in NSTEMI/UA.

Why is this apparent paradox ? What is basic differnce between UA and AMI ?
 In STEMI there is a sudden & total occlusion of a coronary artery usually by a thrombus with or without a plaque .The immediate aim is to open up the blood vessel . Every minute is important as myocardium undergoes a continuous process ischemic necrosis. So thrombolysis (or more specifically fibrinolysis should be attempted immediately) .The other option is primary angioplasty, which will not be discussed here.
In STEMI there is a sudden & total occlusion of a coronary artery usually by a thrombus with or without a plaque .The immediate aim is to open up the blood vessel . Every minute is important as myocardium undergoes a continuous process ischemic necrosis. So thrombolysis (or more specifically fibrinolysis should be attempted immediately) .The other option is primary angioplasty, which will not be discussed here.
The thrombus in STEMI is RBC & fibrin rich and often called a red clot. Number of fibrinolytic agents like streptokinase, Tissue palsminogen activator,(TPA) Reteplace, Tenekteplace etc have been tested and form the cornerstone of STEMI management.The untoward effect of stroke during thrombolysis is well recognised , but usully the risk benefit ratio favors thrombolyis in most situations except in very elderly and previous history of stroke or bleeding disorder.
Unstable angina is a close companion of STEMI . Many times it precedes STEMI often called preinfarction angina. During this phase blood flow in the coronary artery becomes sluggish gradually,and patients develop angina at rest .But unlike STEMI there is never a total occlusion and myocardium is viable but ischemic, and emergency salvaging of myocardium is not a therapeutic aim but prevention of MI becomes an aim. It is a paradox of sorts , even though thrombus is present in UA , It has been learnt by experience thrombolytic agents are not useful in preventing an MI .
Why thrombolysis is not useful in UA ?
1.In unstable angina mechanical obstruction in the form of plaque fissure/rupture is more common than completely occluding thrombus. So lysis becomes less important.
2. Even if the thrombus is present , it is often intra plaque or intra lesional and the luminal projection of thrombus is reduced and hence thromolytic agents have limited area to act.
3.Further in UA/NSTEMI since it is a slow and gradual occlusion (Unlike sudden & total occlusion in STEMI) the platelets get marginalised and trapped within the plaque .Hence in UA thrombus is predominantly white . Often, a central platelet core is seen over which fibrin clot may also be formed.
4.All available thrombolytic agents act basically as a fibrinolytic agents, and so it finds difficult to lyse the platelet rich clot.There is also a small risk of these agents lysing the fibrin cap and exposing underlying platelet core and trigger a fresh thrombus.This has been documented in many trials( TIMI 3b to be specific) So if we thrombolyse in UA , there could be a risk of recurrent ACS episodes in the post thrombolytic phase.
5. UA is a semi emergency where there is no race against time to salvage myocardium .Administering a stroke prone thrombolytic agent tilts the risk benefit ratio against it.
6. Among UA, there is a significant group of secondary /perioperative UA due to increased demand situations. Here there is absolutely no role for any thromolytic agents, the simple reason is , there is no thrombus to get lysed.
7.Many of the UA patient have multivessel CAD and might require surgical revascualarisation directly .
So fibrinolytic agents are contraindicated in UA so what is the next step ?
The emergence of intensive and aggressive platelet-lytic agents.
A combination of aspirin, clopidogrel, heparin, glycoprotien 2b 3a antagonist formed the major therapeutic protocol in these patients.Even though these are called antiplalet agents some of them like 2b/3a antagonist eptifibatide, tirofiban, and many times even heparin has a potential to dissolve a thrombus. So technically one can call these agents as thrombolytic agents.
What are the unresolved issues
Even though clinical trials have convincingly shown thrombolytic agents have no use in UA .There is a nagging belief THAT there could be group of patients with UA , still might benefit from thrombolysis as total occlusions have been documented in some cases with UA.This is especially true in peri-infarction unstable angina (Pre & post) as there is a fluctuation between total and subtotal occlusions ) .But bed side recognition of this population is very difficult.
Many would consider this issue as redundant now, since most of these patients are taken up for emergency revascularisations
Posted in Cardiology - Clinical, cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, angioplasty, aspirin, bmj, cardiology, clopidogrel, clot, coronary thrombosis, drsvenkatesan, eptifibatide, fibrinolytics, fuster, heparin, jacc, lancet, madras medical college, nejm, nstemi, pci, platelet, ptca, red clot, reteplace, stemi, streptokinase, thrombolytic agents, tisue plasminogen activator, tnk tpa, tpa, unstable angina, virchow, white clot | 9 Comments »
September 8, 2008 by dr s venkatesan
Diuretics are the most commonly prescribed anti hypertensive agents.Thiazide diuretics which was introduced many decades ago , lost popularity in recent years , again got a second life after the publication of ALLHAT trial recently. Now diuretics has become the the drug of first choice in almost any hypertension unless any specific contraindication.
The most commonly used thaizide is hydrochlorthiazide ,and chlorthalidone.The blood pressure reducing effect is so consistent and smooth , all the currently popular molecules like ACE inhibitors and ARBs come with a combination with thiazide. While every one is clear diuretics are effective anti hypertensive agent How it does is not clear.

How does a diuretic reduce blood pressure?
A. The exact mechanism is not clear. May not be uniformly effective in all patients with HT.
B . Salt sensitive HT respond well to diuretics.
C. Volume correction /free water clearance might be a factor
D. Direct effect on vascular smoth muscle documented.The sodium transporter is blocked and hence calcium : sodium exchange is prevented .This depletes intracellular calcium in vascular smooth muscle cells .Less calcium for actin myosin interaction and hence vasodilatation
E. Thiazides combine well with all other antihypertensive drugs (ACEI, ARB, Beata blockers, calcium blockers)
F. Loop diuretics like frusemide can never be a good antihypertensive agent.
Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged acei, allhat, ARBS, diuretics, drsvenkatesan, hypertension, jnc7, lancet, loop of henle, reanl hypertension, salt sensitive, sodium, thiazide | Leave a Comment »
September 7, 2008 by dr s venkatesan

Chronic renal failure and CAD are common companions.Severe CAD in patients with renal failure pose an imposing task on the treating physicians.CABG and kidney transplantation both are major interventions.When a patient requires both the decision making becomes much more difficult.
The possible choices are
A. Do CABG first follow it with renal transplant .
B. Do renal transplant first follow it with CABG.
C. Do CABG first and defer transplant & advice life long dilaysis
D.Do renal transplant and offer medical management / PCI for CAD if feasible.
E.Simultaneous CABG & renal transplant is a remote possibility .
F.In terminally ill , combined cardiac and renal transplantation is the ultimate option. (Possible in very few centres in the world)
G.In severe co-morbid condtions avoid both and support life. Success is not in completing the procdeures but in providing useful life !
Among the options the most prefered worldwide is option no 1. This has a caveat. If angina is dominant CABG should precede transplant. If cardiac failure is dominant the issue need further scrutiny.
Given a situation ( DCM & End stage renal disese) , your patient could undergo only one procedure, which will you prefer ?
This again is highly emprical but logic could still be applied. Never do CABG with a sole aim of improving severe LV dysfunction in ischemic DCM .It happens only in journal articles & major clincal trials!.Of course mitral valve correction and LV reduction surgery might help.But in a patient with renal failure prolonging the CABG on table time , with add on surgery is highly risky. So it would be logical to think intensively for postponement of the CABG in a patient with class 4 cardiac failure and renal failure. Do only the transplant .
What is the impact of end stage renal failure on LV dysfunction ?
End stage renal failure has a great adverse impact on LV function. Many times it is reversible.We will never ever know, if you do a CABG first on them. So always think twice or even thrice before voting on this vital issue . Correction of renal impairment can improve the cardiac status dramatically in some.
Posted in Cardiology - Clinical, cardiology -Therapeutics, cardiology- coronary care, Uncategorized | Tagged cabg, cardiology, cardiomyopathy, combined cabg and renal transplant, dialysis, drsvenkatesan, end stage renal failure, kidney international., nejm, pci, renal transplant | Leave a Comment »
September 7, 2008 by dr s venkatesan
CURRENT CARDIOLOGY PRACTICE: EVIDENCE OR EXPERIENCE BASED ? AN ANALYSIS OF ACC/AHA GUIDELINES.
S. Venkatesan, Madras Medical College. Chennai
If a major therapeutic procedure is adviced based on simply by experience or expert opinion how can we say evidence based medicine is practiced !
Evidence based cardiology is the buzz word in global cardiovascular health care organizations. All diagnostic and therapeutic interventions are undergoing rigorous randomized trials for proof of efficacy and safety.  ACC/AHA have published management guidelines and it has been accepted as de-facto standard of clinical cardiology practice world wide. In these guidelines class 1 indication is defined as Conditions for which there is evidence for and/or general agreement that the procedure is useful and effective. These indications are supported by three levels of evidence.(A,B,C) .It has been observed, many of the recommendations in class 1 were supported by only level C evidence. (Expert consensus or agreement ). We analysed how much of todays guidelines is agreement based and how much is evidence based. The latest practice guidelines of ACC/AHA for Acute myocardial infarction , Unstable Angina and Non–ST-Segment Elevation Myocardial Infarction , chronic stable angina ,coronary angiography were analysed. The no of class 1 indications were counted in each set of guidelines and each of the indication were sub grouped with reference to the levels of evidence to which it was supported. There were a total of 210 class 1 indications.
ACC/AHA have published management guidelines and it has been accepted as de-facto standard of clinical cardiology practice world wide. In these guidelines class 1 indication is defined as Conditions for which there is evidence for and/or general agreement that the procedure is useful and effective. These indications are supported by three levels of evidence.(A,B,C) .It has been observed, many of the recommendations in class 1 were supported by only level C evidence. (Expert consensus or agreement ). We analysed how much of todays guidelines is agreement based and how much is evidence based. The latest practice guidelines of ACC/AHA for Acute myocardial infarction , Unstable Angina and Non–ST-Segment Elevation Myocardial Infarction , chronic stable angina ,coronary angiography were analysed. The no of class 1 indications were counted in each set of guidelines and each of the indication were sub grouped with reference to the levels of evidence to which it was supported. There were a total of 210 class 1 indications.
|
|
Class 1
Level A
|
Class 1
Level B
|
Class 1
Level C
|
P value
1A vs 1C
|
|
AMI(54)
|
7
|
25
|
22
|
<.0001
|
|
UA (66)
|
11
|
26
|
29
|
<.0001
|
|
CSA(59)
|
8
|
29
|
22
|
<.0001
|
|
CAG(31)
|
3
|
12
|
16
|
<.0001
|
|
Total(210)
|
29(13.9%)
|
92(43.8%)
|
89(42.4%)
|
<.001
|
13.9% of class 1 indications were based on level A evidence. 42.4% of class 1 indication were based on Level C ( agreement of experts).Though evidence based cardiology is considered to define the standards in Cardiology practice in reality we lack evidence in most of the situations.
We conclude that consensus or agreement based cardiology practice is the dominant theme in current ACC/AHA
Posted in Cardiology -Interventional -PCI, cardiology-ethics, Infrequently asked questions in cardiology (iFAQs) | Tagged Add new tag, american college of cardiology, bmj, cardiology, cardiosource, coronary, ebm, evidence based medicine, guidelines, lancet, md consult, nejm, pci, unstable angina, who | Leave a Comment »
« Newer Posts - Older Posts »












{kind=link}
{kind=link}
{kind=link}
{kind=link}